
 It’s not news to anyone that the opioid drug problem within America has become a major health crisis. So much so, that the Opioid Epidemic Commission, chaired by Governor Chris Christie (NJ), is now urging the White House to declare this epidemic a state of emergency. With 142 Americans dying every day from opioid-related overdoses, our country is “enduring a death toll equal to September 11th every three weeks,” the commission tells us.
It’s not news to anyone that the opioid drug problem within America has become a major health crisis. So much so, that the Opioid Epidemic Commission, chaired by Governor Chris Christie (NJ), is now urging the White House to declare this epidemic a state of emergency. With 142 Americans dying every day from opioid-related overdoses, our country is “enduring a death toll equal to September 11th every three weeks,” the commission tells us.
As these grave statistics loom over our heads, our policymakers scramble to provide solutions. Ironically enough, their solution comes in the form of an opioid. Ten years ago, most people had never even heard of Suboxone or buprenorphine. Now, many of our politicians, reporters, advocacy groups, and doctors refer to these medications as “the most effective form of therapy.” Some have even went as far to say, “medication-assisted treatment is the gold standard of opioid addiction treatment.” While the numbers continue to skyrocket, it makes sense as to why so many are now leaning on medications such as Suboxone, Vivitrol, and Probuphine to “do the trick.”
Nevertheless, let’s call a spade a spade.
By referring to these medications as the “most effective form of treatment,” rather than harm-reduction, we open ourselves up to a wave of misguided supporters. Addicts and their families have and will continue to turn to these modalities for a solution, because after all, they were told these medications would help. Unfortunately, what they are experiencing is NOT what they were promised.
Rather than becoming free from the burden of addiction, countless MAT patients find themselves in a deeper hole than when they began.
A Firsthand Experience With Probuphine
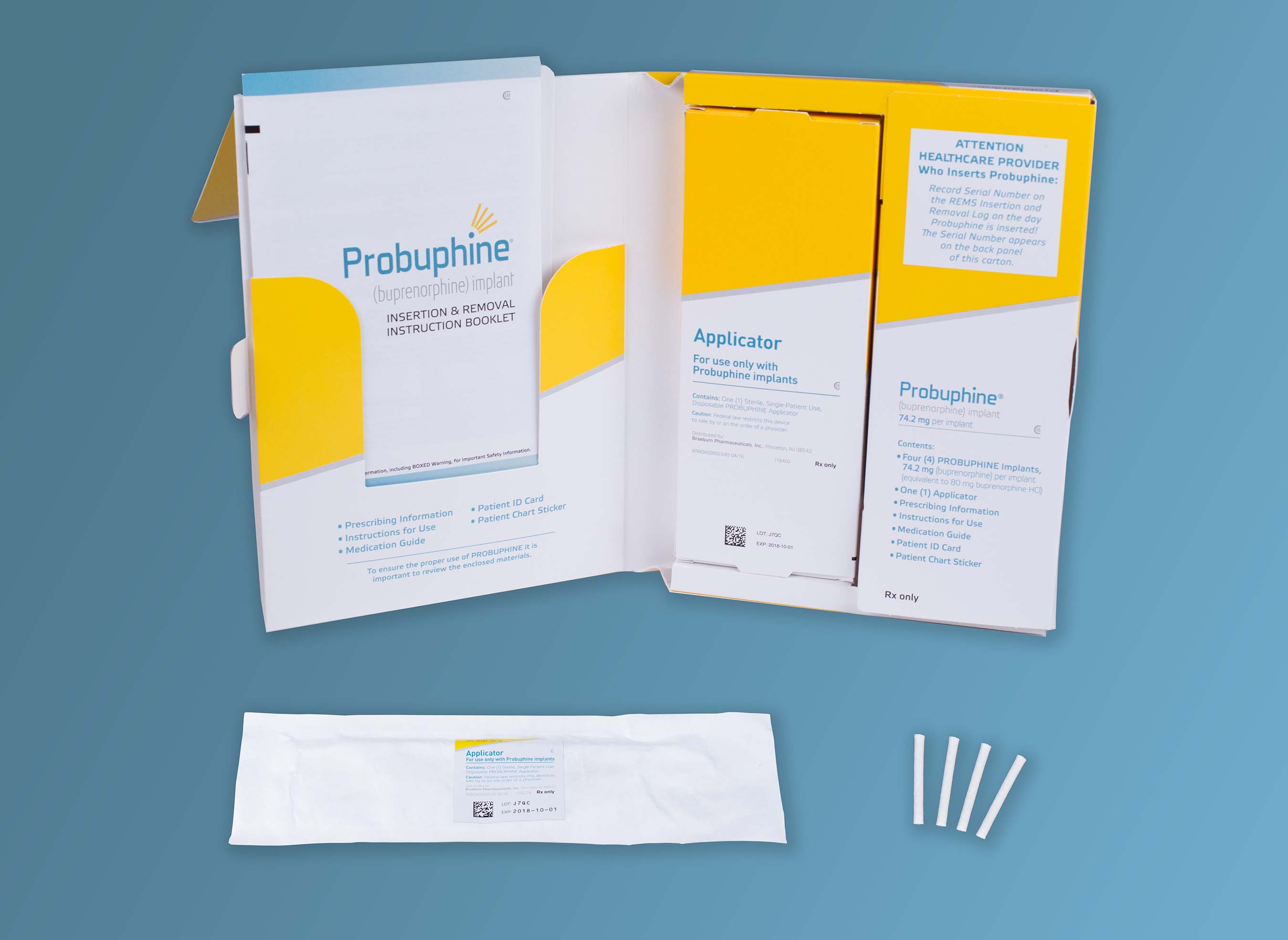
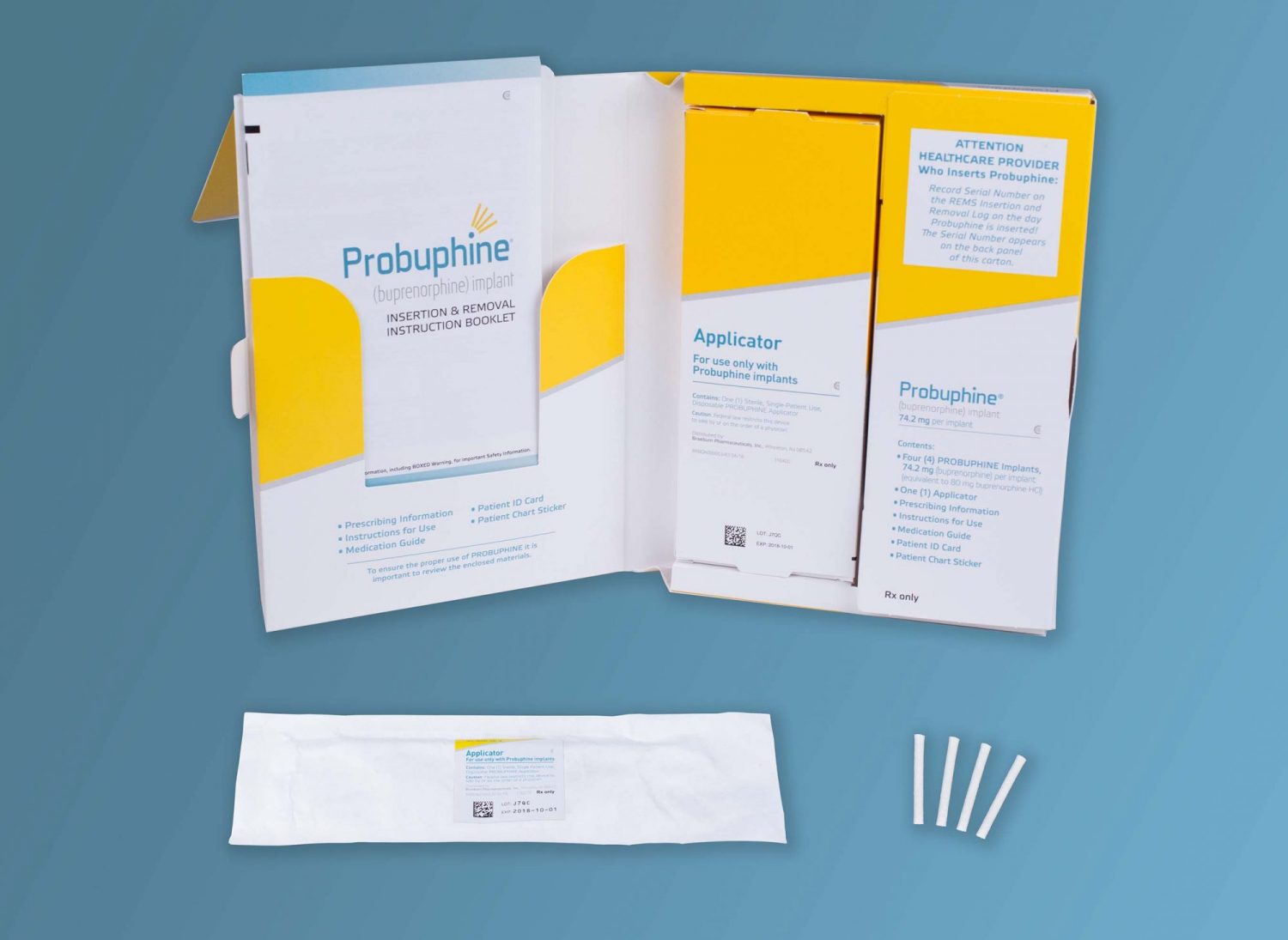
Last year the FDA approved the first buprenorphine implant, Probuphine. Since its approval, advocates have raved about this medicine being the future to addiction treatment, even some calling it a “revolutionary game-changer.” But, what if we told you not much has changed? Recently, we heard the story of a local woman, and her personal experience with Probuphine. After completing a detoxification program, this young woman had the buprenorphine implant placed in her arm for continued treatment. Nevertheless, after the implantation, the patient did not receive stabilization or ongoing therapeutic services and counseling. For some, this may be confusing since the modality is referred to as medication-assisted treatment, but in regards to Probuphine, doctors who administer the drug are only required to see their patients every 6 months.
As many would assume, without the proper clinical interventions and care, the young woman went on to use heroin again, while having the Probuphine still implanted. Surprisingly though, she did not experience precipitous withdrawal from this interaction, which is supposed to occur when heroin, or other opioids, are used in conjunction with buprenorphine.
This antagonistic reaction is the major incentive for using the Probuphine implant to reduce abuse and/or mixed use of opioids. Without it, many users will have no reason to stop abusing drugs like heroin or OxyContin. In fact, without the fear of withdrawal in place, Probuphine removes the consequences for the addict and instead gives them the opportunity to use freely without the fear of feeling “dopesick.” Now, when the individual runs out of their drug of choice, they have an implant to lean on, until they can score their next high. Coincidentally enough, this was the experience of this particular woman, who reveled in her newfound “freedom.”
This terrifying reality has us pose the question, is this modality really treatment, or even harm reduction for that matter?
It seems the more suitable name for this “game-changer” is medication-assisted addiction.
A Contradiction To Probuphine
When we visit the website for Probuphine, we find an extensive report on prescribing information and directions for Probuphine. As one would assume, the report details clinical trials, efficacy of the drug, and indications and usage. Similar to any other medication, the manufacturers must include adverse reactions, contradictions, and so on. Some of them include the possibility of precipitous withdrawal, abuse and dependence, neonatal opioid withdrawal syndrome, and infections and complications associated with the implant.
Nevertheless, what we found interesting was the section titled Continuation of Therapy. This section outlines what to do if, and when, treatment needs to be continued. In other words, when a patient needs another 6-month regiment of Probuphine. Isn’t the primary purpose of Probuphine to stop the use of opioids after 6 months? Why would someone need a second round of the medication? The section then goes on to say, “If new implants are not inserted on the same day as the removal, patients should be maintained on their previous dose of transmucosal buprenorphine (i.e., the dose from which they were transferred to PROBUPHINE treatment) prior to additional PROBUPHINE.”
One may wonder why a previous dose of transmucosal buprenorphine is necessary after 6 months, especially if it is only for one day. It’s simple. Buprenorphine is addictive, especially after long-term use. The makers of Probuphine have laid out these instructions, because they already know there is a high likelihood that the patient will experience withdrawal. So, we ask, what exactly is the end goal? Six months, a year, two years; what happens to the patient after the final implant is removed? More than likely, they will have to enter a residential program, where they can be medically supervised for withdrawal symptoms and provided clinical care to counteract the obsessions and cravings associated with addiction.
Couldn’t we have just done that in the first place?
A Hidden Agenda
Earlier in this article, we mentioned that the Opioid Epidemic Commission is now urging the President to declare the addiction and overdose problem in our country a state of emergency. Along with this suggestion, the panel has also released an interim report of recommendations for the White House to consider. Many of their recommendations are necessary in fighting this crisis, including equipping all law enforcement with Naloxone, improving prescriber education, and addressing the issue of synthetic opioids being smuggled into our country. Nonetheless, there is one that may in fact only add to our troubles.
One suggestion within the report proposes that the White House establish and fund better access to medication-assisted treatment, seeing as only 10% of those addicted to opioids are receiving this form of care. The panel even goes as far to suggest that ALL treatment facilities offer medication-assisted treatment, such as buprenorphine, within their modalities and philosophies. But, what if there was more to the story then meets the eye?
The panel consists of five members, with Governor Chris Christie (NJ) as chair. Alongside him, you have Governor Charlie Baker (MA) and Governor Roy Cooper (NC), both states which have been hit especially hard by the opioid crisis. Bertha Madras, a psychobiology professor at Harvard University also takes seat on the panel. And lastly, you have Patrick Kennedy, former Congressman from Rhode Island and paid spokesperson for Advocates for Opioid Recovery. Kennedy has made it his personal mission to advocate for those in need of treatment. Ironically enough, new reports tell us that Advocates for Opioid Recovery has received “charitable donations” of $900,000 from Braeburn Pharmaceuticals, the maker of Probuphine. Kennedy is also a board member of CleanSlate, a treatment provider that primarily utilizes medication-assisted treatment, such as Probuphine.
Furthermore, each member has strongly supported the utilization and expansion of medication-assisted treatment, so while this panel itself can be considered bipartisan, their approach is nothing short of biased. With that in mind, it is fair to assume that addiction treatment will no longer be an individualized practice. Rather than assessing the patient and their specific needs, our government would rather pigeonhole addicts into a subcategory of “less-fortunates,” who’s only hope is based upon which medication will work best. What happened to doing no harm? Or, explaining all of the options to the patient? Instead, they hide behind statistics that say people don’t die on buprenorphine, conveniently forgetting to mention the potential of abuse and addiction, and for what? A possible pay out?
A Sad Reality
The state in which we find ourselves is truly a sad reality. Thousands of Americans are dying from an addiction that was created by drugs like OxyContin and Vicodin. And now, our government wants us to believe that the only way to solve such a problem, is by prescribing more medication.
We are not naïve. We understand that medication-assisted treatment can and has been necessary for some individuals, and without it, they may have become another statistic. But, by saying things like “medication-assisted treatment is the gold standard for addiction treatment,” people then assume it is the be-all-end-all, in terms of treatment. We are basically telling families and addicts that their chances of recovery are slim, and their only hope of staying sober is dependent on their willingness to take another addictive medication.
If that were at all true, fellowships like Alcoholics Anonymous and Narcotics Anonymous wouldn’t exist; treatment providers that still believe in an abstinence-based model of treatment would go out of business. And, the millions of people who have found recovery through TOTAL abstinence, would all return back to active addiction.
Contact Clearbrook Today
Were you promised a life free from the cycle of addiction, but you still feel and think the same way you did when you were getting high? Have you found yourself addicted to a medication that was supposed to help? Did someone tell you that your best chance toward a life of recovery was through taking a medication? If so, you should know there is another solution, and it can be found at Clearbrook Treatment Centers.
For 45 years, we have been providing effective drug and alcohol treatment to the chemically dependent person, through the utilization of an abstinence-based model of care. By doing so, we have had the privilege to watch countless individuals rebuild their lives and restore their relationships. If you or someone you know is currently caught in the grips of addiction, please do not wait any longer. Please contact our Admissions Specialists today and see what recovery has to offer.
ARE YOU OR SOMEONE YOU CARE ABOUT STRUGGLING WITH DRUGS OR ALCOHOL?
CALL CLEARBROOK TREATMENT CENTERS NOW AT 1-800-582-6241



{kind=link}